
You might be sitting at your kitchen table right now with a sketch on a napkin, a half-built CAD file, and a quiet belief that your device could help real people.
Then the doubts creep in.
Is this a company, or just an expensive science project? Am I crazy for trying to build a startup medical device from the Midwest, far from the usual coastal noise? How do I avoid burning years on the wrong thing?
I know that feeling. I’ve had the late nights, the stomach-drop moments, and the “head in hands” pauses where everything feels heavier than it should. Medtech doesn’t hand out easy wins. But it does reward founders who stay honest, stay disciplined, and stay close to the core problem.
This is the guide I wish more people had given me straight. No glossy founder theater. No fake certainty. Just the hard parts, the shortcuts that matter, and the human support you’ll need when the work gets lonely.
The Hard Truth About Building a Startup Medical Device
You spend six months building a prototype. A surgeon likes the concept. A hospital innovation team takes the meeting. Then the challenging work starts. Design controls, test plans, reimbursement questions, supplier problems, and a bank account that starts looking thinner every month.
That is the business.
A startup medical device company asks more of you than a typical startup. Patients can get hurt if you cut corners. Buyers need more proof before they change behavior. Progress often feels slow because hardware, documentation, testing, and clinical input all have to line up at the same time.
Many first-time founders underestimate what they’re starting. They think they’re building one product. They’re really building four companies that have to mature together:
- A device: It has to solve the problem reliably.
- A quality and regulatory system: Your records, process, and traceability have to hold up under scrutiny.
- A commercial business: Someone has to buy it, use it, and get value from it.
- A founder support system: You need enough emotional stability, peer support, and honest feedback to keep going when nothing seems to move.
That last one gets ignored, especially by smart, proud founders in the Midwest. We tell ourselves we can grind through it. Bad idea. Medtech has too many long stretches where you feel stuck, underqualified, or alone. Find other founders early. Find operators who have shipped hard products. Find people you can call during the head in hands moments before you make a desperate decision.
If you have not done the work to validate a startup idea before you build, stop pretending you have a company. You have a hypothesis with expenses.
My blunt advice is simple. Do not romanticize medtech. If you want quick experiments and cheap mistakes, build software. If you still feel called to build a medical device, good. Commit with your eyes open. Respect the process. Ask for help early. Stay close to real clinicians, real buyers, and real peers who will tell you the truth.
You can recover from being early. Sloppy execution is harder to survive.
Find a Real Problem Before You Build Anything
You drive to a hospital at 6:15 a.m., wait outside the staff entrance with a coffee going cold, and walk in convinced your device idea is brilliant. By noon, a charge nurse has shown you the taped-up workaround her team already uses, a materials manager has told you nobody owns the budget, and a physician has shrugged because the problem annoys them but does not change patient outcomes.
That is a good day.
It is far better to get your ego bruised in discovery than to spend two years building something nobody needs badly enough to adopt.
A lot of startup medical device founders start with the object. The sensor. The attachment. The dashboard. The algorithm. Then they try to force reality to match the prototype. Healthcare does not reward that kind of optimism. It buries it under workflow, budget constraints, clinical skepticism, and plain old inertia.
In the Midwest, I see another layer. Founders are practical, proud, and slow to ask for help. They keep polishing the idea in private because they do not want to look naive in front of clinicians or investors. That instinct costs you time. Get out of the building early. Bring the half-baked questions. Let people who live the problem show you where the core pain sits.
Stop pitching and start investigating
Your job in early conversations is simple. Shut up and learn.
Do not ask, “Would you use this?” That question invites politeness. Ask for a recent, specific failure. Ask what happened next. Ask who had to clean it up. Ask what it cost in time, money, stress, or patient risk.
Use questions like these:
Start with the broken moment
“Tell me about the last time this went wrong.”Get out of theory fast
“What did your team do in that moment?”Find the fallout
“Who felt the pain most?”Trace the money
“Does this create delays, waste, denials, overtime, or rework?”Find the current workaround
“What are you using today because the current process is not good enough?”
That last answer matters more than compliments. Workarounds are evidence. If a unit has built a spreadsheet, laminated cheat sheet, or hallway ritual to survive a problem, you are finally near something real.
What strong signal sounds like
You are listening for friction, not praise.
Good signs:
- Repeated pain: “This happens every shift.”
- Local hacks: “We made our own process because the official one slows us down.”
- Clear owner: “Operations cares about this.” “Nursing leadership tracks it.” “Supply chain gets blamed.”
- Emotional charge: “People hate this.” “Patients get confused.” “Everyone dreads discharge because of it.”
Weak signs:
- Polite interest: “Interesting.”
- Vague approval: “I could see that.”
- Idea shopping: “Can it also do these six other things?”
- No buyer in sight: The user is mildly annoyed, but nobody controls budget or feels urgency.
A nice idea is easy to compliment. A painful problem creates stories, workarounds, and visible frustration.
Score the problem before you score the product
Founders love to rate features. Rate the problem first.
Use a simple scorecard:
| Dimension | What you're looking for |
|---|---|
| Pain | Does this create stress, delay, risk, or wasted labor? |
| Frequency | Does it happen often enough to matter? |
| Budget owner | Can you identify who would pay to fix it? |
| Behavior change | Will your solution fit existing workflow, or force people to relearn too much? |
Healthcare is brutal on products that demand too much behavior change for too little gain. If your device asks busy clinicians to add steps, log into another system, or change handoff habits, the upside has to be obvious and immediate.
Be hard on yourself here. If the pain is real but the buyer is fuzzy, keep digging. If the buyer is clear but the pain is occasional, keep digging. If both are weak, kill the idea.
Talk to enough people to hear the same problem in different words
One enthusiastic interview means nothing.
You want the same core pain repeated by nurses, physicians, techs, administrators, and buyers inside the same care setting. The wording will change. That is fine. In fact, it helps. Clinical staff may describe the safety risk. Admin may describe throughput. Finance may describe waste. The overlap is where your opportunity lives.
This is also where community helps you stay honest. Bring your notes to another founder. Call an operator who has sold into hospitals. Ask someone local to rip apart your assumptions before you spend on design work. During the head in hands moments, borrowed clarity is worth a lot.
If you need a simple way to pressure-test your early assumptions, use this framework for how to validate a business idea before you build.
My advice
Do not fall in love with being the founder who has a medtech idea. Fall in love with understanding a painful problem better than anyone else.
If people are not frustrated, improvising, and pushing for relief, keep looking. The Midwest gives you an advantage here. You can build real relationships with clinicians, hospital operators, and other founders who will tell you the truth without the coastal theater. Use that advantage.
Kill weak ideas early. Save your energy for the problem people already feel in their bones.
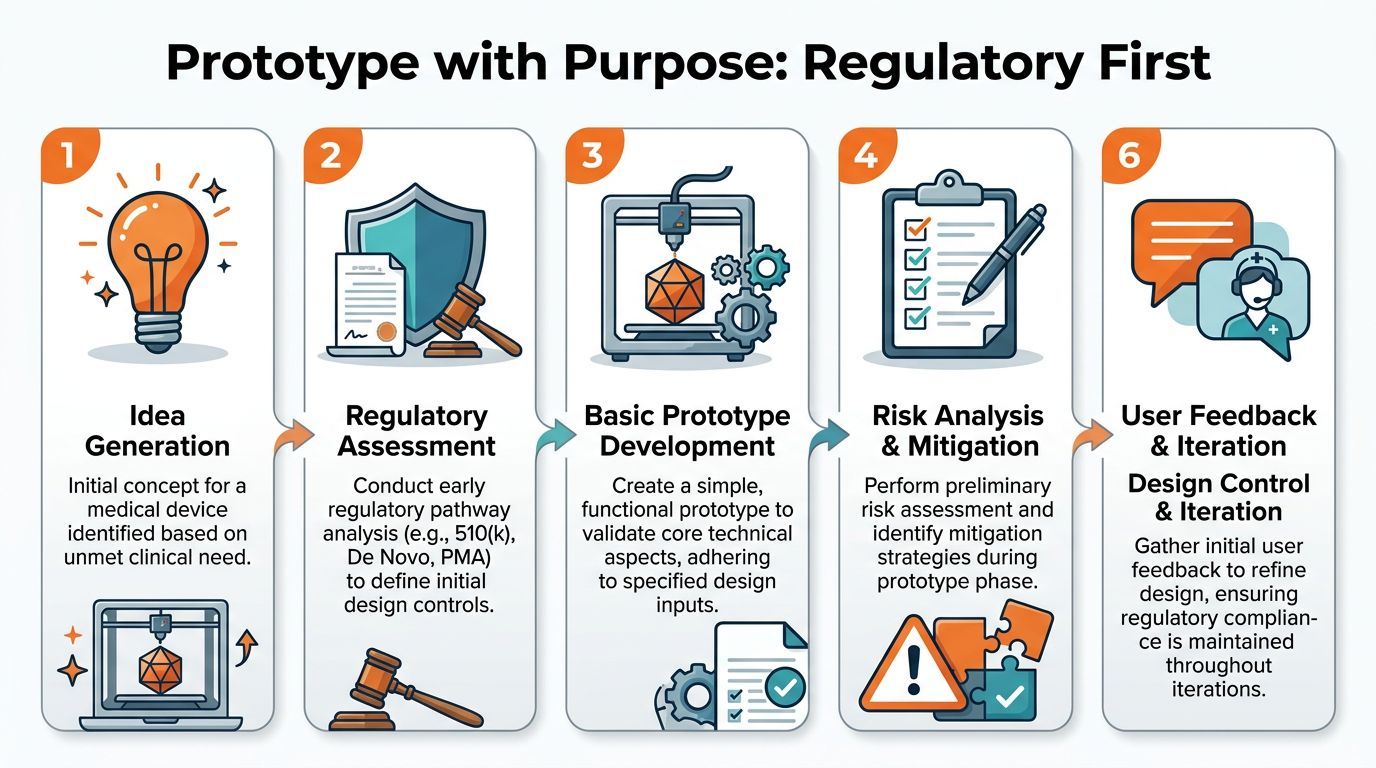
Your First Prototype and Why Regulatory Starts Now
A founder in Chicago spends six months building a slick prototype, gets a few polite investor nods, then hears the sentence that wrecks the quarter: “You need to redo this with regulatory in mind.”
I have watched that happen. It is painful, expensive, and avoidable.
Your first prototype is not a pitch prop. It is the start of your product record. The choices you make here shape your testing plan, your risk file, your quality system, and eventually your path to market. If you treat prototyping like pure invention and save regulatory for later, you create rework when your team is already tired and low on cash.
Build like someone will audit your reasoning
Founders get in trouble because they focus on the object and ignore the decision trail behind it.
You need both.
A good early prototype shows what you built and why you built it that way. It ties back to a user need. It records the main risks. It shows what you tested, what failed, and what changed. That discipline does not slow you down. It protects you from rebuilding the same device twice.
Here is the plain-English version of design controls:
- Design inputs define what the device must do for the user
- Design outputs show the specs, drawings, code, and parts you created
- Verification checks whether you built it to spec
- Validation checks whether it solves the actual user problem in the actual setting
- Risk management documents how someone could get hurt, use it wrong, or misread it
If this feels heavy, keep it light and consistent. A scrappy startup can do this in shared docs, version control, and simple review notes. Sloppy thinking is the burden.
Your first prototype should answer one hard question
Do not cram every idea into version one.
That is ego disguised as speed.
Your first prototype only needs to answer the next question that matters most. Can the sensing method work at all? Can a nurse use the handle with gloves on? Can the device sit in a crowded room without messing up workflow? Pick one or two core uncertainties and attack those first.
That usually means one of these:
- a rough functional prototype to test the core mechanism
- a usability model to test handling, labeling, or setup
- a workflow mockup to see how the device fits into care delivery
- a software simulation to test logic before hardware is locked
If you need a practical way to scope that work, this guide to prototyping and product design for early-stage founders is a good place to start.
Learn your risk class before you spend real money
You do not need to become a regulatory expert this week. You do need a rough read on the kind of device you are building.
A lower-risk product usually gives you more room to learn cheaply. A moderate-risk device demands tighter documentation, better testing, and fewer sloppy assumptions. A high-risk device can consume years, serious capital, and emotional stamina that many first-time founders underestimate.
My advice is blunt. If you are a new founder with limited capital, do not wander into a high-risk category by accident. Choose your lane on purpose.
This is one place where Midwest founders can make faster progress than they think. You can sit down with a local quality lead, a hospital operator, or another medtech founder who already paid the tuition on these mistakes. Buy them coffee. Show them your prototype notes. Ask where your assumptions break. Those conversations can save months.
A prototype checklist that keeps you honest
Before you approve another build, write down the answers to these questions:
- What exact assumption are we testing with this version?
- Who is the intended user?
- Where will they use it?
- What could go wrong during normal use or misuse?
- What evidence will we collect from this round?
- What did we change from the last version, and why?
- What must stay flexible, and what are we now locking down?
If your team cannot answer those questions clearly, you are not running a prototype cycle. You are burning money in a machine shop.
My strongest recommendation
Pair your technical builder with someone who cares about quality and risk from day one. This can be a consultant, an experienced advisor, or a sharp operator in your founder circle who knows regulated products.
You do not need bloated process. You need clean habits.
The founders who survive medtech are not the ones with the prettiest first prototype. They are the ones who keep learning without losing the thread. On the hard nights, the head in hands nights, that thread matters. So do the people around you who can look at your messy draft, your failed test, your half-baked risk table, and say, “Good. Now fix this part next.”
Demystifying the FDA and Clinical Evidence
You’re sitting in a hospital conference room in Milwaukee or Indianapolis. A clinician likes the problem you’re solving. Your prototype finally works well enough to demo. Then someone asks the question that tightens your chest.
“What’s your regulatory path, and what evidence do you have?”
That is the moment the dream gets real.
Founders often treat FDA strategy like paperwork they can outsource later. That is a mistake. Your pathway shapes your product, your study plan, your budget, your timeline, and who will even take your call.
The FDA is not a black box. It is a system with rules, categories, and evidence expectations. If you respect that early, you save yourself from expensive fantasy.
One reason this feels heavy is that many teams are not prepared. Only 16% of pre-commercial firms feel highly prepared for the U.S. Quality Management System Regulation, based on the industry readiness data cited in this 2025 medtech discussion. If you get serious here before your peers do, you create an advantage.
The three main paths
You do not need to memorize the whole CFR on day one. You do need to understand which bucket you are walking toward.
510(k) is the familiar route
Use this path when you can show your device is substantially equivalent to something already on the market.
That does not mean easy. It means clearer. You still need solid testing, clean documentation, and a believable argument that your device is as safe and effective as the predicate.
A lot of Midwest founders like this route because it feels financeable. I get it. Investors and early commercial partners usually prefer a path they recognize. Just do not confuse familiar with cheap or fast.
De Novo is for real novelty with manageable risk
This path fits devices that are new but do not belong in the highest risk class.
De Novo can be a smart strategic choice. It can also become a vanity move. If your team cannot explain, in plain English, why the novelty matters to patients or clinicians, you are probably adding risk without adding value.
I’ve seen founders fall in love with being first. Hospitals do not pay extra because you were first. They pay when the product solves a painful problem and survives scrutiny.
PMA is the hardest route
PMA usually applies to high risk devices, and it changes the whole company.
The timeline gets longer. The evidence burden gets heavier. The capital needs get much larger. As noted earlier in this guide, this route can consume years and an amount of money that breaks underplanned startups.
If your device belongs here, face that fact early. Build the company around it. Do not drift into PMA because nobody did the classification homework.
A quick comparison
| Path | Best fit | What founders like | What founders hate |
|---|---|---|---|
| 510(k) | Similar to an existing device | Clearer route | Documentation burden and regulatory cost |
| De Novo | Novel lower to moderate risk device | Strategic differentiation | More uncertainty |
| PMA | High-risk device | Strong moat if you survive | Long timeline, heavy evidence, brutal expense |
Documentation is part of the product
I want to be blunt here. If it is not documented, it does not exist in any way that helps you with regulators, investors, diligence, or future teammates.
Your regulatory file is the legal memory of your company.
Write down:
- User requirements
- Design decisions
- Risk assessments
- Test methods
- Test results
- Version history
- Clinical rationale
That sounds tedious because it is. It also keeps your company from collapsing into tribal knowledge. In small startup teams, especially in Midwest ecosystems where everyone wears three hats, people rely on memory and hallway conversations. Then someone leaves, a file goes missing, or an investor asks why a design choice changed. Now you have a trust problem.
Clean records calm chaos.
Clinical evidence is a sequence, not a single giant trial
Many founders make one of two mistakes. They either underthink evidence, or they assume they need a blockbuster clinical trial from day one.
Both instincts waste time.
Your clinical evidence plan should answer a narrower question: what evidence do we need now to reduce the next meaningful risk?
Sometimes that means bench testing. Sometimes it means usability work, human factors input, literature support, clinician interviews, or a focused clinical study. The right sequence depends on the device, the setting, and the regulatory path.
What matters is order.
Start with the evidence that removes the next doubt
I’d look at four categories first:
- Usability evidence: Can the intended user operate it correctly and safely?
- Workflow evidence: Does it fit the actual care environment?
- Performance evidence: Does it do what you claim it does?
- Safety evidence: Where can it fail, and how will you show that risk is controlled?
That workflow point gets ignored all the time. A device can perform beautifully in a lab and still die on a hospital floor because it slows the nurse down, creates confusion, or adds another training burden no manager wants.
That is why founder community matters more than people admit. On your worst nights, the head in hands nights, another medtech founder can save you months by telling you, “We already made that mistake in a cath lab in Peoria. Fix the handoff step before you spend money on a study.”
Here’s a useful explainer before you get too deep into pathway choices:
What I’d do if I were starting today
I’d pick the least painful route that still supports a real business.
Then I’d build the evidence plan backward from the next value inflection point. Not from what sounds impressive in a pitch. From what gets the company to the next honest milestone.
Ask three questions:
- What does FDA need next?
- What does a credible clinical champion need next?
- What does an investor need to believe next?
Those answers will not match perfectly. Your job is to bring them as close together as possible.
The part founders avoid
Teams rarely fail here because they are dumb. They fail because they postpone clarity.
They avoid the classification question. They avoid the ugly usability test. They avoid writing down decisions because the sprint feels more urgent. Then the bill comes due.
Face the hard facts early. Ask better questions. Find operators who have already lived through the mess. In the Midwest, that support is closer than founders think, and you will need it.
The companies that survive medtech are usually the ones that stop arguing with reality and start building around it.
Making It Selling It and Getting Paid
Friday afternoon. A surgeon likes your device. The pilot went well. Your team walks out feeling ten feet tall.
Then purchasing asks for unit economics. Operations asks who will service it. Finance asks which budget owns it. Revenue cycle asks how the hospital gets paid. Suddenly the deal that felt real turns into a pile of unanswered questions.
That is normal.
Getting a startup medical device into the market is not a single win. It is three jobs at once. You have to make it consistently, sell it to institutions that hate surprises, and show how money flows after the sale. Midwest founders usually learn this the hard way because local hospitals will give you honest feedback fast. If you are smart, you will treat that as a gift, not rejection.

Manufacturing without building a factory
Do not rush to build manufacturing in-house.
Early on, you need repeatable output, quality discipline, and fast feedback from people who have seen production fail before. A good contract manufacturer can give you that. A bad one will drain cash, miss deadlines, and create quality problems that show up in the field.
I would screen for four things first:
- Process control: Can they hit tolerances consistently, not just on a good day?
- Change discipline: Can they document process changes and tell you what changed, when, and why?
- Quality maturity: Can they work inside your quality requirements without acting annoyed every time paperwork appears?
- DFM feedback: Can they tell you which parts of your design will break production before you learn it through scrap and delays?
Founders sometimes treat manufacturing like a vendor relationship. It is not. It is a trust test. Visit the floor. Meet the people who will build the product. Ask how they handle deviations. In the Midwest, you can often drive to your manufacturer and look them in the eye. Do that.
Reimbursement is the fuel
A common mistake is assuming buyers will pay solely because the product is useful.
Healthcare does not reward usefulness by itself. It rewards budget fit, billing fit, workflow fit, and political fit inside the institution. A clinician can love your device and still fail to get it approved because nobody can explain who pays, who benefits, and how the purchase gets justified.
Your economic story needs to be simple enough that a busy department leader can repeat it without you in the room.
| Question | Why it matters |
|---|---|
| Does it save staff time? | Time savings can turn into labor savings or more patient capacity. |
| Does it reduce complications, readmissions, or downstream cost? | That gives clinical and financial stakeholders a reason to care. |
| Does it fit existing reimbursable care? | Products that ride on current billing patterns face less resistance. |
| Who owns the budget? | A user is not always a buyer. You need to know who signs. |
If you cannot explain the financial case in a few plain sentences, you are not ready to scale sales.
Do not ask a hospital to admire your invention. Give them a reason to approve the purchase.
Selling to hospitals is committee work
Hospital sales are slow because hospitals are protecting themselves. That is not bureaucracy for its own sake. It is the system doing what it was designed to do.
One person almost never gets you to a signed deal. The physician may want it. Nursing may worry about training. Supply chain may push for standardization. IT may get involved if software touches any system. Finance may want proof the economics hold up outside a pilot.
So prepare for the room, not the champion.
What I’d have ready before outreach
- Clinical case: What problem do you solve in ordinary care, not in a perfect demo?
- Workflow case: What changes for staff on day one?
- Economic case: Why should this get funded now?
- Proof package: Testing, documentation, quality materials, pilot plan, and implementation basics
A lot of early founders pitch the device itself. Mature founders pitch the adoption path.
That shift matters. Buyers are not purchasing your engineering effort. They are deciding whether your product creates a manageable change inside an already overworked system.
My advice on commercialization
Sell the easy install first.
If your startup medical device requires major behavior change, heavy training, shaky reimbursement, and a painful procurement process at the same time, you built yourself a trap. Strip out friction wherever you can. Make training shorter. Make setup simpler. Tighten the economic story. Choose the first customer segment with the fewest approval layers.
I also want founders to stop isolating themselves during this stage. Commercialization is where confidence gets punched in the mouth. You miss a quarter. A pilot stalls. A hospital goes quiet after acting excited for weeks. Those are real head in hands moments. Talk to operators who have lived them. In Chicago and across the Midwest, those people are more accessible than many founders realize, especially if you spend time with the local venture capital community in Chicago and the builders around it.
The companies that get paid are usually not the ones with the flashiest technology. They are the ones that make adoption feel safe, practical, and worth the hassle.
Getting Funded and Finding Your People in the Midwest
A startup medical device eats money long before it earns trust.
That’s why I get irritated when founders parrot coastal startup advice that doesn’t fit medtech. “Raise fast, grow fast, figure it out later” is a cute slogan until regulation, testing, and quality punish every lazy shortcut you took.
I think Midwest founders have a hidden edge. Not because the work is easier here. Because the noise is lower, the relationships are more real, and too many people still underestimate the local funding paths sitting right in front of them.
Stop acting like only coastal money counts
National grants and big-name investors matter. Of course they do.
But many founders skip local and state-level support because it doesn’t feel glamorous. That’s foolish. According to this 2025 medtech funding guide focused on startup financing options, SBIR grants have a 15-20% success rate, regional programs can be less competitive for early validation, and only 20-30% of eligible startups access them.
That tells me two things.
First, there’s neglected money on the table. Second, founders who do the boring work can create a real advantage.
My funding stack for an early Midwest medtech founder
I wouldn’t start with VC unless the situation clearly calls for it.
I’d build a capital stack in layers.
Layer one is non-dilutive money
I'd start by looking here.
- State grants and local programs: Illinois and Midwest programs can help fund feasibility, prototyping, and early validation.
- Research and development credits: These won’t solve everything, but they can reduce burn.
- University-linked programs: If you have technical or clinical ties, these can open doors.
This kind of money buys time without forcing you into an overpriced round too early.
Layer two is angels who understand hard things
Not all angel money is equal.
You want investors who understand that medtech progress looks lumpy. The wrong angel expects software speed. The right angel understands why a regulatory milestone or pilot design matters more than vanity metrics.
Layer three is venture capital
VC can be powerful. It can also distort your judgment if you raise before your fundamentals are real.
If you want a broader sense of the overall situation, this overview of venture capital in Chicago is useful context. But my main advice is simple. Don’t chase VC just because it feels like the “real startup” move.
Sometimes the strongest founder move is staying lean long enough to earn better terms later.
What medtech investors actually want
A lot of founders pitch medtech like consumer tech. Bad move.
Investors in this space usually care about a different mix:
| What they want | What it signals |
|---|---|
| Clear clinical problem | You’re solving something painful, not ornamental |
| Credible regulatory plan | You won’t get blindsided by the process |
| Evidence path | You know how to reduce risk step by step |
| Commercial logic | There’s a believable path to getting paid |
| Focused founder | You won’t burn cash trying to impress everyone |
If your deck screams “look how advanced our technology is” but whispers about pathway, workflow, and payment, you’re not ready.
Midwest founders don’t need more hype. They need cleaner strategy and better capital discipline.
The Midwest advantage nobody talks about enough
In the Midwest, people will still tell you the truth if they respect you.
That matters more than founders admit.
In some scenes, everybody performs confidence. They nod through weak ideas, make soft intros, and disappear when the work gets ugly. That environment can kill a founder slowly because you don’t get clean feedback until it’s expensive.
Here, if you build trust, you can often get straighter answers from operators, clinicians, manufacturers, and early backers. That’s gold.
Your real moat is people who tell you the truth
I need to say this plainly. The lonely nights are not a side issue. They are one of the core risks.
A startup medical device company puts you under weird pressure. You carry technical stress, money stress, timeline stress, and identity stress all at once. If you do that alone for too long, your judgment gets worse.
You need a small group of people who can do three things:
- Challenge you without ego
- Share tactics without posturing
- Stay steady when your confidence dips
Not a giant networking event. Not a room full of service providers handing out cards. A trusted handful of builders who’ve had their own “what am I doing” moments.
The kind of support I’d build around myself
I’d want:
- One regulatory-savvy advisor who can tell me when I’m making an avoidable mistake.
- One technical peer who understands hardware pain.
- One commercial operator who thinks in buyers and budgets.
- A few founder friends with whom I can be frank when things are rough.
That support system won’t replace execution. But it will keep you from spinning out.
And in my experience, that saves more companies than another polished pitch deck ever will.
Your Journey as a Kind Bold Founder
Building a startup medical device will test parts of you that a normal job never touches.
It will test your patience when progress is slow. It will test your humility when users don’t care about the feature you loved. It will test your courage when the money gets tight and the path gets foggy.
That’s normal.
What matters is how you build. Solve a real human problem. Respect the process. Stay honest about risk. Ask for help before panic makes you stupid. Keep your standards high and your ego low.
I care a lot about the kind of founder who wins.
Not just smart. Not just ambitious. Kind. Bold. Hard-working. The kind of person who wants to build wealth and impact without turning into a taker. The kind of person who can be vulnerable enough to say, “I’m stuck,” and strong enough to keep going after hearing the truth.
That founder has a shot.
If you’re in the Midwest, don’t apologize for building from here. Use the advantages. Stay practical. Build relationships that are real. Let the coasts chase status. You chase substance.
Medtech is hard. Good. Hard work filters out tourists.
If this path still feels worth it to you after reading all that, then you’re probably built for it.
If you want a room full of kind, bold, hard-working founders who share real tactics instead of fake networking energy, take a look at Chicago Brandstarters. It’s a free vetted community for Chicago and Midwest builders who want honest support, small private dinners, and the kind of friendships that help you survive the brutal parts of entrepreneurship.
Leave a Reply